I’ve never tried this, but advice I’ve seen online is if your doctor won’t order testing, ask them to note in your chart that they are declining testing. Apparently the implicit threat of a lawsuit if they’re wrong is enough to kick at least some of them into CYA mode.
Pharmacist and 4th year medical student here. Medical tests are ordered based upon their statistical ability to alter your likelihood of a diagnosis. No test is perfect in either direction (negative result meaning you don’t have disease or positive result indicating you have disease). Tests cost money, take resources of the healthcare system, and have the potential to be wrong. When a test is wrong, it can result in financial, emotional, and physical harm to an individual.
Example: you’re an otherwise healthy 34 year old and you feel a little under the weather and are coughing. It’s only been going on a few days, mild fever, but you’re worried and you go to the doctor. Your doctor thinks this is most likely a viral infection, recommends Tylenol and ibuprofen and sends you home. You imply to the doctor you’ll sue if you don’t get antibiotics and a chest x-ray just to be safe. The doctor, rather than argue with you when they have a dozen other patients to see, just orders the stuff and moves on. The chest X ray doesn’t explain your cough, but there’s a small lesion of undetermined significance on the X-ray. Now you need a CT. The CT says “probably a self-limited granuloma from a fungal infection, can’t rule out cancer, correlate with biopsy”. Then you have to go get sedated, put a camera down your throat, and have a pulmonologist take a sample of your lung to see if you have cancer. Maybe you end up with a complication from the sedation or a pneumothorax. Meanwhile the antibiotics you took didn’t really improve your cough but now you have this uncomfortable itchy rash. Are you allergic to the amoxicillin? Or did you just develop the typical rash seen in people who have mononucleosis that also take amoxicillin? Will you get allergy testing for the amoxicillin? Just avoid amoxicillin, an awesome antibiotic, for the rest of your life?
We are restrictive in our prescribing of medications and tests not because we don’t care about you, not because we want to save the hospital or the insurance company money (in fact the hospital prefers we order more things because they make money on testing). We are restrictive because we want to maximize benefit while minimizing risk, and everything we do has risks and benefits.
Not to mention, the entire medical system does NOT want to prescribe antibiotics - especially cutting edge ones - unnecessarily, in the interest of dragging out the emergence of antibiotic-resistant strains as long as possible. Some pathogen (commonly, though not exclusively, staph) somewhere will eventually mutate into a resistant strain to some particular antibiotic. This is extremely problematic, because it means that the antibiotic becomes essentially ineffective at eradicating that mutation of the pathogen. If this occurs with a cutting edge antibiotic, and the pathogen happens to be a strain that’s resistant to many other antibiotics, you get what’s called a “superbug”; in the worst case, you’re all the way back to “get some rest, stay hydrated, and good luck”.
This is actually true. We have an over testing problem in the western world and it does cause some people harm, at least in the form of stress and anxiety caused by believing you have something that you don’t (due to false positives), or in some cases in the form of unnecessary operations and their associated medical risk.
And that’s without getting into the financial impacts, whether that be an impact on an individual or, in a civilised country, on the government.
That’s obviously not to say that nothing should be tested. Only that tests should be limited to cases with a heightened risk, be it someone showing symptoms (as OP obviously was, which is why this general problem of over testing is not applicable in this case) or being part of a demographic know to have heightened risk, as determined by experts and medical best practices.
Yeah, great question, I don’t understand it either, but marginalized groups like women or people of color can have a hell of a time getting medical professionals to take their concerns seriously. Maybe it’s just a hubris thing. “How dare this person question my judgment when I’m the doctor?”
I mean, there are tons of studies on racial and gender inequality in healthcare, but OK, go off.
For example, members of minority groups have longer wait times in the ER [7-9], are less likely to receive catheterization when identical expressions of chest pain are presented [10], and are less likely to be recommended for evaluation at a transplant center or be placed on a transplant waiting list when suffering from end-stage renal disease [11]. African Americans receive lower-quality pain treatment [12, 13], even when covered by the same medical insurance [14, 15] and seeking treatment at the same emergency department [16] as patients of other races. (https://journalofethics.ama-assn.org/article/education-identify-and-combat-racial-bias-pain-treatment/2015-03)
“I was told I knew too much, that I was working too hard, that I was stressed out, that I was anxious,” said Ilene Ruhoy, a 53-year-old neurologist from Seattle, who had head pain and pounding in her ears.
Despite having a medical degree, Ruhoy said she struggled to get doctors to order a brain scan. By the time she got it in 2015, a tennis ball-sized tumor was pushing her brain to one side.
[…]
Since the data has been collected from white majority countries, and I’d be very surprised to see the same trend in, say, China - I think it reflects basic tribalism more than anything.
Still a problem if you’re part of a minority group anywhere, but I genuinely think it’s a fundamental human characteristic.
The medication thing is because the trials are overwhelmingly run on white men aged 18-30. You can imagine the outrage if we’d been selectively testing on minorities, and women of childbearing age are avoided to protect any unborn children.
Complex topic, but these things don’t always come down to calculated racism. And yet there is that kernel of truth in it that people don’t want to confront, which is that humans have this basic level of racism “baked in” to the hardware. Tricky.
On top of that, I’m sure unhelpfully paternalistic and sexist attitudes do persist in medicine. Anecdotally, this can be particularly severe in Indian cultures - I couldn’t believe how differently a female friend was treated by the same doctor.
Edit: oh yeah, sorry, what I meant to say is only white people are capable of doing wrong.
The research is out there with a quick search. As a white woman though, I definitely don’t need research to know it’s true. Especially with gynecological issues, pain levels, and psychiatry. We’re “hysterical,” and though they don’t use that word anymore, that judgement is alive and well.
Well I’m guessing that the healthcare will pay it. And at least in Switzerland, the healthcare can announce official that they won’t pay anymore for anything that one doctor decides/order. So if the doctor orders to many thing, that the healthcare has to cover, then he soonly will lose his job. So in this way the doctor will only order stuff that are really needed and maybe won’t make a test against cancer (but this happens not really often)
Else if the customer has to pay, then yes it would be stupid to not let the customer do the test.
There are some tests that can do harm to patients. In this case obviously a CT scan should have been ordered immediately, but not every pt with a cough needs a fat dose of radiation.
That’s terrible advice. I don’t know if any doctor that is “out to get you” by not ordering tests. Tests are not harmless. Improper testing can kill you. For example, you have a headache with no red flag symptoms. You keep pushing, some doctor orders an MRI and now you have what we call an incidentaloma. Some incidental mass that isn’t going to cause you any issue and is unrelated to your headache. Now you latch on to this abnormal thing, you worry about it, it affects your life. More scans and tests are done to figure out what this is. Eventually a biopsy is offered. Good news, it’s just some normal cells that happen to look funny on MRI, but completely benign. Bad news, the biopsy had complications and now you’re wheelchair bound for the rest of your life.
It’s thoughts like this where the “advocate for yourself” has turned into the “threaten the person that dedicated multiple decades of their life to help others to get what you want” that has lead to the insanely piss poor defensive medicine in the United States.
Tldr: refer every patient and order every tests until someone dies of bankruptcy or an unecessary complication because webmd.
Bad news, the biopsy had complications and now you’re wheelchair bound for the rest of your life.
how often does this actually occur? I assume if they’re doing biopsies of brain material there’s a risk but seems like it’s a low probability if they’re biopsi-ing your liver…
Also, when physicians find something wacky or unusual, is there any desire to do more imagine to see if that’s the only oddness? for example, I had a retrocecal appendix (discovered during my appendectomy) - is that the only thing going on that’s funky / unusual, or should I check / have imagine for other stuff? My docs didn’t have a consistent answer - one said yeah, one said nah, one said it’s nbd but if it was their appendix they might ask for other tests. :|
Fortunately my insurance is about as likely to pay for extra stuff as it is to cut my copay to zero, so it’s not an issue I can address, but it does hang around in the back of my head.
Not frequent, but enough to make you question are we truly doing no harm when we indulge people. Medicine is an art, at the end of the day its a mix of statistics and experience. Not everything has a clear cut or even a right or wrong answer. Do this long enough, and you’ll see things that have minimal risk turn into a clusterfuck.
For your question, yes I’ve seen minor things end up killing someone through sheer bad luck things can spiral out of control despite all the right steps being taken. Hence the inherent risk they mention of death during all informed consents.
That advice was born from women minorities struggling to get doctors to take their concerns seriously. Look, I get that medicine is a risk/benefit analysis, but patients also need some level of recourse if they aren’t being listened to. I can’t imagine what it would feel like to be pushing for tests because you know something is off, only to finally be tested and told it’s too late, maybe if it was caught sooner. Yet, we know this happens. We also know that women and minorities receive demonstrably different care. That fact alone shows there are plenty of situations where a patient may need to fiercely advocate for themselves and question their doctors’ judgment.
I’m not saying completely ignore medical professionals and scream “lawsuit” because google. However, you live in your body and understand your own baseline more than anybody. Sometimes you absolutely can tell if something is truly wrong. Personally, I learned the difference between bad pain and there-is-something-fucking-wrong-you need-to-go-to-the-ER pain in my early 20s when I had ovarian torsion. Thankfully, I was at one of the best hospitals in the country, got a CT scan, and was in surgery lickety split. However, I met someone who had pretty much the exact same symptoms and story and ended up losing an ovary because she was sent home from the ER with them telling her it was normal cramps & anxiety.
Ultimately, imo it should be about informed consent. If you’ve gotten the same answer from 5 doctors and you still want the biopsy, despite the risks that have been plainly laid out for your, then fine. If you end up paralyzed, then you have to deal with the consequences of your decision.
I’m well aware of those biases, and I practice with the thought of always assume the patient is right and telling the truth. However once all the initial testing, exam, records scream negative, now you have someone that the best course of action is to help them understand they are not sick and truly healthy to avoid unecessary tests and complication. Surprisingly, some don’t like to hear that they are fine and healthy. Some Psych patients have much higher mortality, not because of being ignored, but because of over testing and complications.
FYI, finding an incidentaloma and doing another scan 3 months later to see that it’s disappeared is also life saving. My mother had a lung problem, got some imaging done, they found a lump in her lung, and instead of going directly to poking it for a biopsy or surgery, they checked 4 months later, and saw that it resolved on it’s own. If it was cancer, they would have seen changes in it, and known it was something to be investigated further at the time of the second scan. Doctors need to manage expectations and refer people for therapy if they have anxiety around their health.
Oh for sure, my comment is more towards people that won’t accept the diagnosis of everything is fine and no further testing is needed. Those people tend to yell, sue, go find some other doc, try chi blocking and crystals before they will talk to a therapist about their anxiety.
My comment about incidentaloma is more when you find something that wasn’t causing any true issue. Now what. You have to get another scan. But before that, there was no indication that anything was wrong because nothing was wrong. Now you’re stuck working and monitoring something that ends up being benign and would have been that way if you never look.
Same with any tests, there’s a rate of false positive to be aware of. When your suspicion is high, it outweighs it, but when it’s low and the test comes back positive, your stuck now and are often obligated to do unecessary work to prove that it was a false positive.


{kind=link}
I’ve never tried this, but advice I’ve seen online is if your doctor won’t order testing, ask them to note in your chart that they are declining testing. Apparently the implicit threat of a lawsuit if they’re wrong is enough to kick at least some of them into CYA mode.
On that note, why would they decline tests in the first place? You’re the one paying.
Pharmacist and 4th year medical student here. Medical tests are ordered based upon their statistical ability to alter your likelihood of a diagnosis. No test is perfect in either direction (negative result meaning you don’t have disease or positive result indicating you have disease). Tests cost money, take resources of the healthcare system, and have the potential to be wrong. When a test is wrong, it can result in financial, emotional, and physical harm to an individual.
Example: you’re an otherwise healthy 34 year old and you feel a little under the weather and are coughing. It’s only been going on a few days, mild fever, but you’re worried and you go to the doctor. Your doctor thinks this is most likely a viral infection, recommends Tylenol and ibuprofen and sends you home. You imply to the doctor you’ll sue if you don’t get antibiotics and a chest x-ray just to be safe. The doctor, rather than argue with you when they have a dozen other patients to see, just orders the stuff and moves on. The chest X ray doesn’t explain your cough, but there’s a small lesion of undetermined significance on the X-ray. Now you need a CT. The CT says “probably a self-limited granuloma from a fungal infection, can’t rule out cancer, correlate with biopsy”. Then you have to go get sedated, put a camera down your throat, and have a pulmonologist take a sample of your lung to see if you have cancer. Maybe you end up with a complication from the sedation or a pneumothorax. Meanwhile the antibiotics you took didn’t really improve your cough but now you have this uncomfortable itchy rash. Are you allergic to the amoxicillin? Or did you just develop the typical rash seen in people who have mononucleosis that also take amoxicillin? Will you get allergy testing for the amoxicillin? Just avoid amoxicillin, an awesome antibiotic, for the rest of your life?
We are restrictive in our prescribing of medications and tests not because we don’t care about you, not because we want to save the hospital or the insurance company money (in fact the hospital prefers we order more things because they make money on testing). We are restrictive because we want to maximize benefit while minimizing risk, and everything we do has risks and benefits.
Not to mention, the entire medical system does NOT want to prescribe antibiotics - especially cutting edge ones - unnecessarily, in the interest of dragging out the emergence of antibiotic-resistant strains as long as possible. Some pathogen (commonly, though not exclusively, staph) somewhere will eventually mutate into a resistant strain to some particular antibiotic. This is extremely problematic, because it means that the antibiotic becomes essentially ineffective at eradicating that mutation of the pathogen. If this occurs with a cutting edge antibiotic, and the pathogen happens to be a strain that’s resistant to many other antibiotics, you get what’s called a “superbug”; in the worst case, you’re all the way back to “get some rest, stay hydrated, and good luck”.
Because tests have harm. The average persone doesn’t understand what the sensitivity and specificity of a test means.
This is actually true. We have an over testing problem in the western world and it does cause some people harm, at least in the form of stress and anxiety caused by believing you have something that you don’t (due to false positives), or in some cases in the form of unnecessary operations and their associated medical risk.
And that’s without getting into the financial impacts, whether that be an impact on an individual or, in a civilised country, on the government.
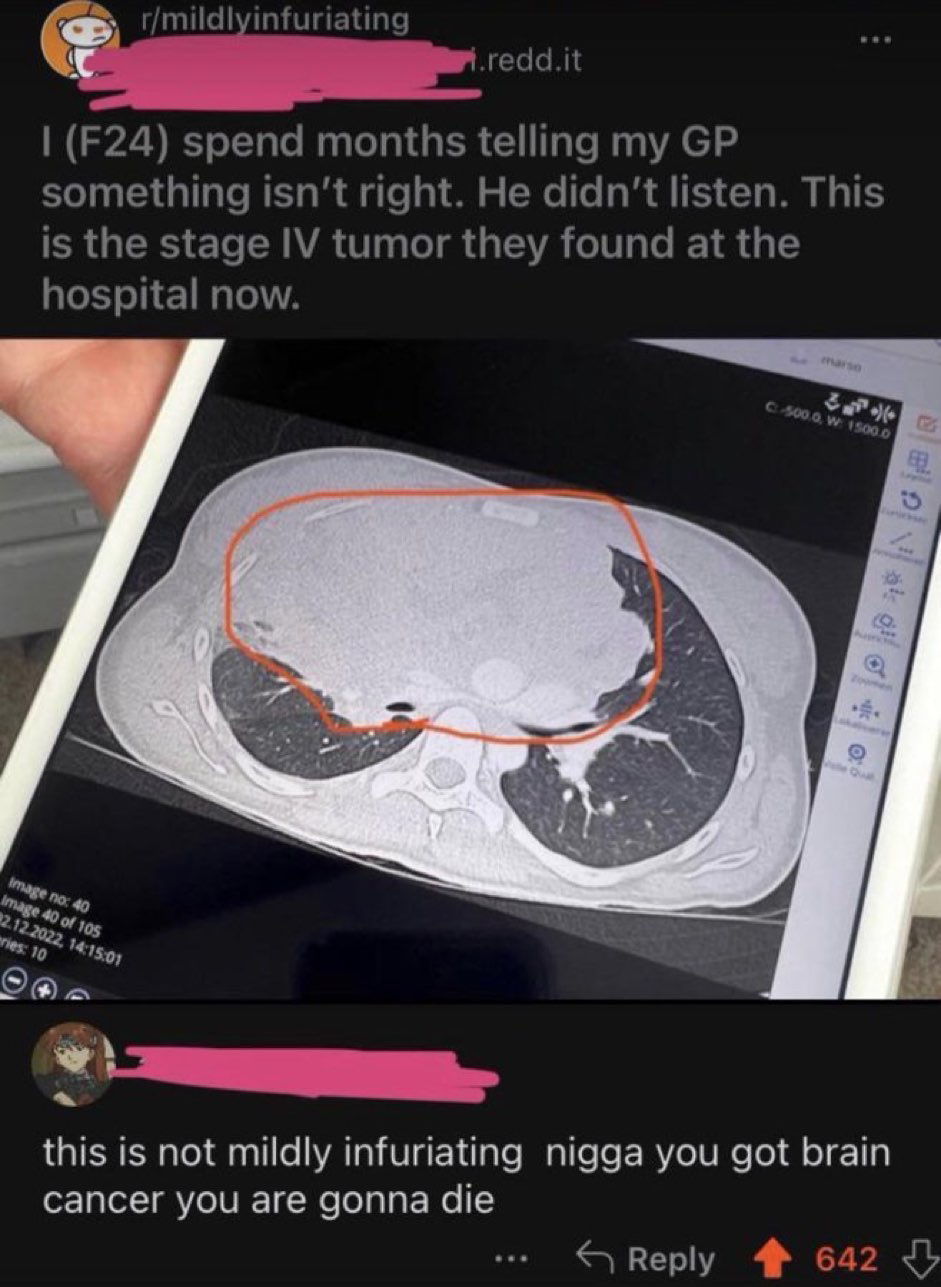
That’s obviously not to say that nothing should be tested. Only that tests should be limited to cases with a heightened risk, be it someone showing symptoms (as OP obviously was, which is why this general problem of over testing is not applicable in this case) or being part of a demographic know to have heightened risk, as determined by experts and medical best practices.
Agreed
Yeah, great question, I don’t understand it either, but marginalized groups like women or people of color can have a hell of a time getting medical professionals to take their concerns seriously. Maybe it’s just a hubris thing. “How dare this person question my judgment when I’m the doctor?”
Removed by mod
Too right! It’s only white men who get the full benefit of modern medical capacity. Everyone else is fucked.
s/ in case it’s needed.
I mean, there are tons of studies on racial and gender inequality in healthcare, but OK, go off.
Can take this too far, though.
Since the data has been collected from white majority countries, and I’d be very surprised to see the same trend in, say, China - I think it reflects basic tribalism more than anything.
Still a problem if you’re part of a minority group anywhere, but I genuinely think it’s a fundamental human characteristic.
The medication thing is because the trials are overwhelmingly run on white men aged 18-30. You can imagine the outrage if we’d been selectively testing on minorities, and women of childbearing age are avoided to protect any unborn children.
Complex topic, but these things don’t always come down to calculated racism. And yet there is that kernel of truth in it that people don’t want to confront, which is that humans have this basic level of racism “baked in” to the hardware. Tricky.
On top of that, I’m sure unhelpfully paternalistic and sexist attitudes do persist in medicine. Anecdotally, this can be particularly severe in Indian cultures - I couldn’t believe how differently a female friend was treated by the same doctor.
Edit: oh yeah, sorry, what I meant to say is only white people are capable of doing wrong.
https://www.hopkinsmedicine.org/news/articles/physicians-more-likely-to-doubt-black-patients
https://www.today.com/health/implicit-bias-medicine-how-it-hurts-black-women-t187866
The research is out there with a quick search. As a white woman though, I definitely don’t need research to know it’s true. Especially with gynecological issues, pain levels, and psychiatry. We’re “hysterical,” and though they don’t use that word anymore, that judgement is alive and well.
Well I’m guessing that the healthcare will pay it. And at least in Switzerland, the healthcare can announce official that they won’t pay anymore for anything that one doctor decides/order. So if the doctor orders to many thing, that the healthcare has to cover, then he soonly will lose his job. So in this way the doctor will only order stuff that are really needed and maybe won’t make a test against cancer (but this happens not really often)
Else if the customer has to pay, then yes it would be stupid to not let the customer do the test.
Possibly Kaiser, or similar, where they’re the ones paying themselves which is somehow legal?
There are some tests that can do harm to patients. In this case obviously a CT scan should have been ordered immediately, but not every pt with a cough needs a fat dose of radiation.
That’s terrible advice. I don’t know if any doctor that is “out to get you” by not ordering tests. Tests are not harmless. Improper testing can kill you. For example, you have a headache with no red flag symptoms. You keep pushing, some doctor orders an MRI and now you have what we call an incidentaloma. Some incidental mass that isn’t going to cause you any issue and is unrelated to your headache. Now you latch on to this abnormal thing, you worry about it, it affects your life. More scans and tests are done to figure out what this is. Eventually a biopsy is offered. Good news, it’s just some normal cells that happen to look funny on MRI, but completely benign. Bad news, the biopsy had complications and now you’re wheelchair bound for the rest of your life.
It’s thoughts like this where the “advocate for yourself” has turned into the “threaten the person that dedicated multiple decades of their life to help others to get what you want” that has lead to the insanely piss poor defensive medicine in the United States.
Tldr: refer every patient and order every tests until someone dies of bankruptcy or an unecessary complication because webmd.
how often does this actually occur? I assume if they’re doing biopsies of brain material there’s a risk but seems like it’s a low probability if they’re biopsi-ing your liver…
Also, when physicians find something wacky or unusual, is there any desire to do more imagine to see if that’s the only oddness? for example, I had a retrocecal appendix (discovered during my appendectomy) - is that the only thing going on that’s funky / unusual, or should I check / have imagine for other stuff? My docs didn’t have a consistent answer - one said yeah, one said nah, one said it’s nbd but if it was their appendix they might ask for other tests. :|
Fortunately my insurance is about as likely to pay for extra stuff as it is to cut my copay to zero, so it’s not an issue I can address, but it does hang around in the back of my head.
Thanks for your insights!
Not frequent, but enough to make you question are we truly doing no harm when we indulge people. Medicine is an art, at the end of the day its a mix of statistics and experience. Not everything has a clear cut or even a right or wrong answer. Do this long enough, and you’ll see things that have minimal risk turn into a clusterfuck.
For your question, yes I’ve seen minor things end up killing someone through sheer bad luck things can spiral out of control despite all the right steps being taken. Hence the inherent risk they mention of death during all informed consents.
That advice was born from women minorities struggling to get doctors to take their concerns seriously. Look, I get that medicine is a risk/benefit analysis, but patients also need some level of recourse if they aren’t being listened to. I can’t imagine what it would feel like to be pushing for tests because you know something is off, only to finally be tested and told it’s too late, maybe if it was caught sooner. Yet, we know this happens. We also know that women and minorities receive demonstrably different care. That fact alone shows there are plenty of situations where a patient may need to fiercely advocate for themselves and question their doctors’ judgment.
I’m not saying completely ignore medical professionals and scream “lawsuit” because google. However, you live in your body and understand your own baseline more than anybody. Sometimes you absolutely can tell if something is truly wrong. Personally, I learned the difference between bad pain and there-is-something-fucking-wrong-you need-to-go-to-the-ER pain in my early 20s when I had ovarian torsion. Thankfully, I was at one of the best hospitals in the country, got a CT scan, and was in surgery lickety split. However, I met someone who had pretty much the exact same symptoms and story and ended up losing an ovary because she was sent home from the ER with them telling her it was normal cramps & anxiety.
Ultimately, imo it should be about informed consent. If you’ve gotten the same answer from 5 doctors and you still want the biopsy, despite the risks that have been plainly laid out for your, then fine. If you end up paralyzed, then you have to deal with the consequences of your decision.
I’m well aware of those biases, and I practice with the thought of always assume the patient is right and telling the truth. However once all the initial testing, exam, records scream negative, now you have someone that the best course of action is to help them understand they are not sick and truly healthy to avoid unecessary tests and complication. Surprisingly, some don’t like to hear that they are fine and healthy. Some Psych patients have much higher mortality, not because of being ignored, but because of over testing and complications.
FYI, finding an incidentaloma and doing another scan 3 months later to see that it’s disappeared is also life saving. My mother had a lung problem, got some imaging done, they found a lump in her lung, and instead of going directly to poking it for a biopsy or surgery, they checked 4 months later, and saw that it resolved on it’s own. If it was cancer, they would have seen changes in it, and known it was something to be investigated further at the time of the second scan. Doctors need to manage expectations and refer people for therapy if they have anxiety around their health.
Oh for sure, my comment is more towards people that won’t accept the diagnosis of everything is fine and no further testing is needed. Those people tend to yell, sue, go find some other doc, try chi blocking and crystals before they will talk to a therapist about their anxiety.
My comment about incidentaloma is more when you find something that wasn’t causing any true issue. Now what. You have to get another scan. But before that, there was no indication that anything was wrong because nothing was wrong. Now you’re stuck working and monitoring something that ends up being benign and would have been that way if you never look.
Same with any tests, there’s a rate of false positive to be aware of. When your suspicion is high, it outweighs it, but when it’s low and the test comes back positive, your stuck now and are often obligated to do unecessary work to prove that it was a false positive.